- Conditions
- Acromioclavicular injury
Acromioclavicular injury
AC joint (sub)luxation
Introduction
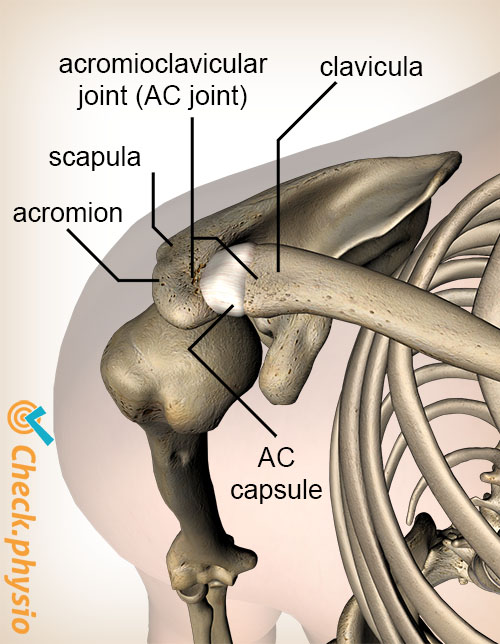
The acromioclavicular joint, also called the "AC joint", forms the connection between the clavicle (collarbone) and the top of the shoulder blade. Dislocation of this joint may cause damage to the ligaments and capsules that stabilize the joint.
Injuries to the AC joint are common in cyclists and judokas. They are at increased risk of falling onto the top of the shoulder. This is a classic cause of acromioclavicular dislocation (luxation).
Description of condition
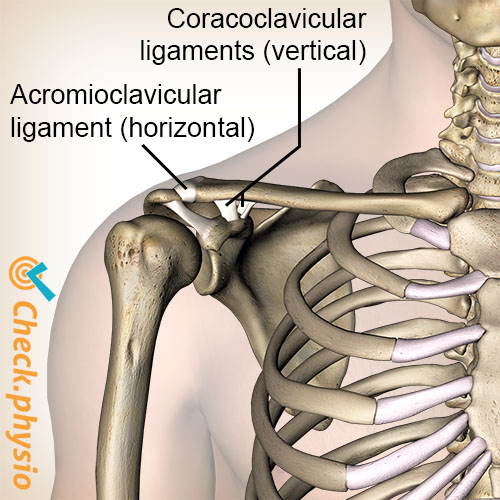
The clavicle is connected to the acromion via the AC joint. This is the top and outermost part of the shoulder blade. The joint is held in position by ligaments. If these ligaments become damaged, this may result in acromioclavicular symptoms.
When the forces on the AC joint become too great, for example through an accident or a fall, this can cause ligament rupture. The clavicle is effectively dislocated.
Cause and history
The injury is usually caused by a fall onto the top of the shoulder or on an outstretched arm. This causes bruising of the surrounding tissues.
Signs & symptoms
The painful spot can often be pinpointed. Sometimes the symptoms can be provoked by pressing on or around the AC joint. The pain increases when the shoulder is moved forward, or when the shoulder hangs down. There may also be swelling.
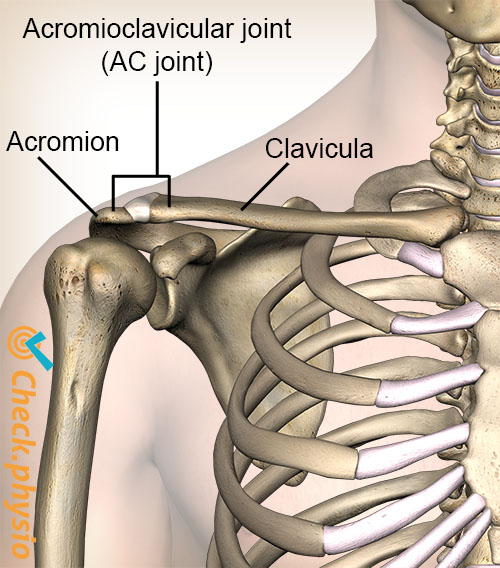
As the AC joint is located close to the surface, it is often clear when there is a severe injury that the clavicle is not in the correct position. The clavicle juts upward slightly and a clear "step" is visible in the shoulder. Always compare the right and left shoulders in order to assess any abnormality.
Diagnosis
A diagnosis is made based on the patient's story and a number of physiotherapy tests. Often passive movement of the upper arm in front of the body toward the chest (horizontal adduction) is painful.
Treatment and recovery
Treatment depends on the type of injury. Types I and II are always treated without surgery. Types IV to VI do require surgery. The treatment of type III is less clear. Physiotherapy treatment is often the initial treatment. If the results are not satisfactory, then surgery will be performed after all.
Rest, ice and a sling
Types I, II and III, treatment initially consists of rest and ice. Rest is ensured by using a sling. For type I, the use of a sling for a few days is usually sufficient. For types II and III, it may be necessary to put the arm in a sling for 6 weeks.
Physiotherapy
For type I, it is possible to have the arm treated immediately by a physiotherapist. Strength exercises can start after a few days. Once full mobility and strength have been regained, all activities can be resumed.
For type II and III, physiotherapy can start after 14 to 21 days. In the case of a serious dislocation of the collarbone, treatment can only start after 6 weeks. Taping may provide extra rest for the AC-joint, if necessary. The ligaments will be fully restored after 8 to 12 weeks. Heavy lifting or exercising is only allowed after that period of time. Also this is only allowed once the shoulder can move without any pain.
Surgery
During surgery, the AC joint will be brought back into the correct position and fixed. An artificial ligament is often used in this process to attach it to the shoulder blade via the collarbone. This keeps the collarbone back in the right place.
After surgery, the arm will need to be kept in a sling for 6 weeks. Physiotherapy treatment can start immediately. Complete recovery after surgery takes six months.
Exercises
Take a look at the exercise program with exercises for AC joint injuries.
More info
You can check your symptoms using the online physiotherapy check or make an appointment with a physiotherapy practice in your locality.
References
Nugteren, K. van & Winkel, D. (2007) Onderzoek en behandeling van de schouder Houten: Bohn Stafleu van Loghum.
Schünke, M., Schulte, E. & Schumacher, U. (2005) Prometheus. Algemene anatomie en bewegingsapparaat Houten: Bohn Stafleu Van Loghum.
Moen, M.H., Vos, R-J. de, Arkel, E.R.A. van, Weir, A., Moussavi, J., Kraan, T. & Winter, Th.C. de (2008) De meest waardevolle klinische schoudertesten Sport & Geneeskunde. 2008;4:6-19.